Going far beyond OSHA
Michigan OSHA’s lead standard has very strict exposure limits for pregnant workers. Are OHS pros ready to face a six-fold reduction challenge?
Appendix A to federal OSHA’s 1978 lead standard (current today) provides that blood lead level (BLL) of workers, both male and female, who intend to have children should be maintained below 30 micrograms per deciliter (ug/dL) “to minimize adverse reproductive health effects to the parents and to the developing fetus.” Many OHS pros believed back in the day that a BLL < 30 ug/dL was unrealistic with hierocracy of controls available at the time.
Appendix A to MIOSHA’s (Michigan OSHA) December 12, 2018, lead standard states “The blood lead levels of female workers who are pregnant should be maintained below 5 ug/dL at all times to prevent adverse health effects to the developing fetus.”
History
In 1978, tort liability claims for a child with adverse effects from lead exposure (mother’s BLL are comparable to BLL in the umbilical cord at birth) was uncertain but could be huge. Many employers solved this dilemma by using various means to keep fertile women away from lead exposure – a practice that the U.S. Supreme Court unanimously decided in 1991 (UAW v Johnson Controls) violates the 1978 Pregnancy Discrimination Act.
Women’s advocates in the 1970s -- including U.S. Supreme Court justice Ruth Bader Ginsberg (Notorious RBG) -- crafted the PDA specifically to counter sex discrimination effects anticipated by OSHA’s 1978 lead standard. The PDA’s fetal protection policies created “shock value.” “General concern over unsafe working conditions, particularly when couched within an OSHA framework, would just not cut it.” (See Columbia Law School Paper Number 07-145).
Shock value
Shock value can undermined OSHA’s 40-year-old lead standard. Flint Michigan’s 2014 lead-in-drinking water crisis, that climbed to a National Emergency in 2016, with lawsuits and criminal charges against 15 state employees with EHS accountability, shocked the nation. Michigan’s water quality standards for lead and MIOSHA’s workplace lead rules are now the strictest in the nation. Fed OSHA, NIOSH, and other state OSHA programs, such as Cal-OSHA, cannot be far behind. Look for BLL update proposals from these groups throughout 2019.
Today’s challenge
BLL < 5 ug/dL always for pregnant workers may be unrealistic in workplaces that handle lead. BLL < 5 ug/dL at the 95th percentile may require that the eight-hour time-weighted average for airborne lead to be maintained at 0.5 ug/m3, nanograms/m3 whole number. Air sampling by someone with CIH®-like skills is necessary to avoid false positive/negative results.
Air sampling is preferable to medical surveillance -- venous blood draw required to measure BLL. While MIOSHA addresses pregnant workers, forty-five percent (45 percent) of all pregnancies are unintended. BLL tests for all female workers is not recommended.
Communication
MIOSHA’s lead rules requires at 1910.1025(l)(1)(i) where there is a “potential exposure to airborne lead at any level” employees shall be informed of the contents of Appendix A and B. Any amount of airborne lead, even nanograms per cubic meter, triggers the requirement.
Posting Appendix A and B in the workplace may satisfy that workers are “informed.” Letting workers interpret information alone is not advisable. Appendix B information, for example, discusses why a worker may want to consult an attorney about their legal rights if disease from lead exposure is suspected. “It should be stressed that OSHA is in no way trying to either encourage or discourage claims or lawsuits,” so says Appendix B.
Required lead warning signs (since June 1, 2016) include the term MAY DAMAGE FERTILITY OR THE UNBORN CHILD. “The employer shall ensure that no statement appears on or near any sign required by paragraph (m)(2) which contradicts or detracts from the meaning of the required sign” per 1910.1025(m)(2)(ii) of the lead standard. Fetus and similar terms, therefore, are not interchangeable within context of the standard’s requirements.
What’s not in MIOSHA’s lead standard?
The American College of Occupational and Environmental Medicine (ACOEM) December 2016 Position Statement on Workplace Lead Exposure calls for, “Mandatory medical removal of all pregnant workers and those workers who are trying to become pregnant must occur when BLLs are more than 10 ug/dL.”
The American College of Obstetricians and Gynecologists (ACOG): Women’s Health Care Physicians, likewise, reaffirmed their position in 2018 that Lead Screening During Pregnancy and Lactation calls for “… abatement of exposures” when BLLs are greater than 10 ug/dL.
Chemical manufacturers that comply with EU REACH legislation calculated the BLL DNEL “for female workers of reproductive capacity” at 10 ug/dL. DNELs, with increasing frequency, are appearing on required workplace safety data sheets for chemical products used in the United States. The EPA, CDC and other authorities call for abatement of exposure for pregnant women at 10 ug/dL.
MIOSHA adopted the “reference level” for BLL, not removal level.
What level?
The choice between BLL at 5 ug/dL or 10 ug/dL for pregnant workers is substantial. A linear comparison with airborne values doesn’t exist between the two BLLs. Airborne lead at 0.5 ug/m3 may control BLL at < 5 ug/dL. Airborne lead at 2.1 ug/m3 may control BLL at 10 ug/dL. One control may be unrealistic while the other is challenging, but perhaps doable, with modern hierarchy of controls. Want absolute BLL safety? Then fertile female workers cannot work with any amount of lead.
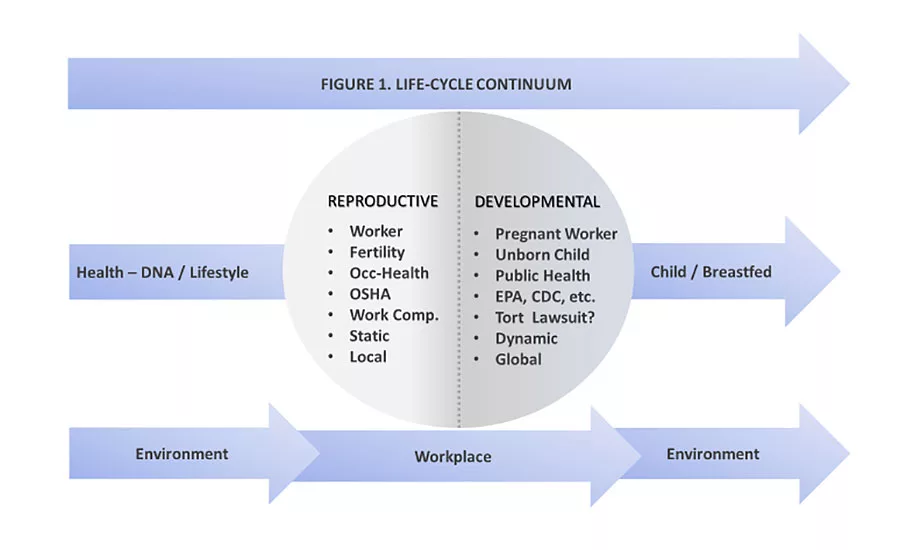
Managing occupational reproductive toxicants (see OSHA 1910.1200 A.7), such as lead, is complex as summarized in Figure 1.
Management of occupational reproductive toxicants should have a weighted influence of 25 percent legal, 25 percent HR, 20 percent committee (Millennial & Gen Z), 20 percent OHS pro, and 10 percent environmental pro. Fifty percent (50%) of weighted influence should include women representation. Consult ACOEM Reproductive and Developmental Hazard Management (2016) and ACOG Employment Considerations During Pregnancy (2018).
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!








